
The Screen That Broke the Trust

Alex has been ill for most of their adult life.
Not visibly ill. Not the kind of ill that people notice on the bus or mention at dinner. The kind of ill that takes decades to name — a slow, grinding battle through misdiagnosis, misunderstanding, and the particular loneliness of knowing something is wrong but not being able to prove it.
Eventually, after years, Alex got a diagnosis. A real one. The kind that comes with a treatment plan, a prescription, and something almost as important as either of those things — a doctor who knew their name, their history, and what a bad week looked like for them specifically.
That relationship took years to build. It was, in its quiet way, a lifeline.

Then the surgery went digital.
The Digital Barrier

The letter arrived explaining that the practice had moved to a new online platform. Appointments, repeat prescriptions, queries, all of it now managed through an app.
Modern. Efficient. Better for everyone.
Except it wasn’t better for Alex.
To request a repeat medication - the same medication, taken for years, prescribed by the same doctor, for the same condition - the process now requires navigating more than ten screens of questions. The questions repeat themselves. They contradict each other. They are written for someone booking a routine check-up, not for someone managing a long-term mental health condition on a difficult morning.
Each screen is another small demand on a person for whom demands are not small.
Each repeated question is a quiet suggestion that the system doesn’t know them, doesn’t remember them, and doesn’t particularly care to.
By the time Alex reaches the end, if they reach the end, more energy has been spent than the task should ever have cost. And there is still no certainty the prescription will arrive.
What used to be a phone call is now an ordeal.
Designing for the “Average”
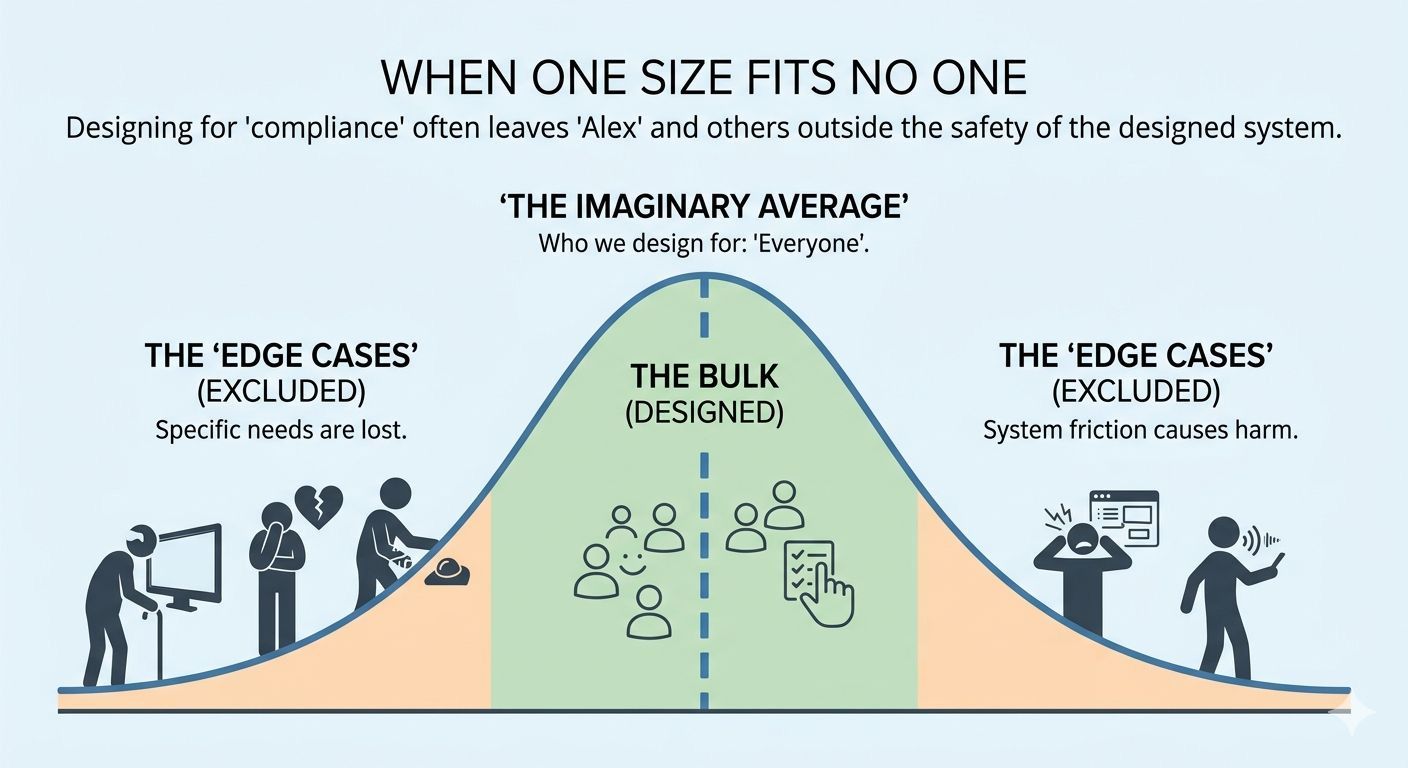
Nobody designed this system to hurt Alex. That’s the thing worth sitting with.
The people who built it almost certainly believed they were making things better. Faster, more consistent, less dependent on the variable quality of a phone call. Easier to scale. Easier to manage. Better for the many.
And perhaps it is better for the many. For someone booking an appointment to discuss a sprained ankle or a blood test result, ten screens might be a minor irritation. A few minutes, a small frustration, forgotten by lunchtime.
But Alex is not the many. One person, with one specific condition, with one set of needs that the system has never once asked about.
This is the problem we keep building into our technology and refusing to look at directly. We design for an imaginary average person who doesn’t actually exist, and we call it progress.
The Framework for Better Tech
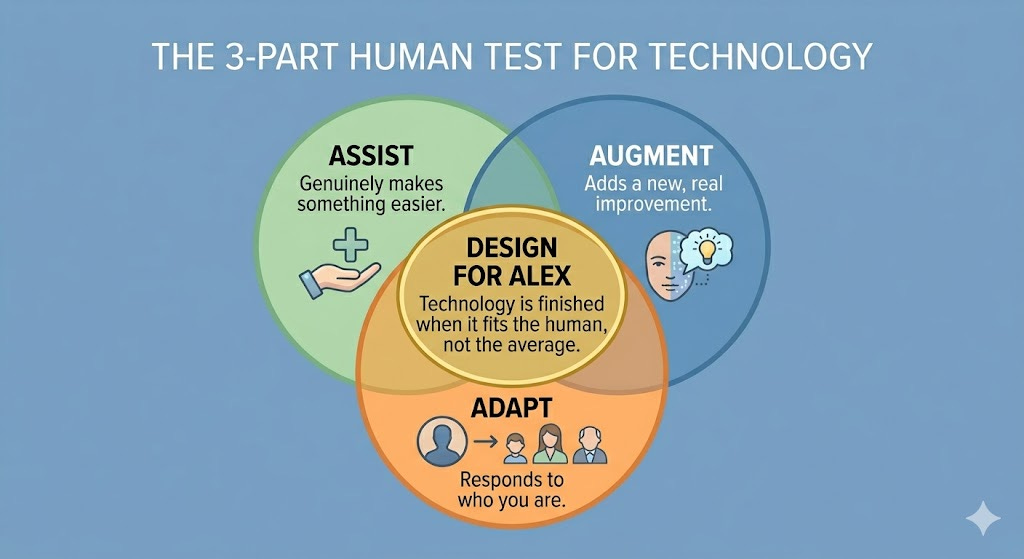
There is a simple test I apply to any technology that is supposed to help people.
Does it assist: does it genuinely make something easier for the person using it, or does it just move the effort around?
Does it augment: does it add something real, something that wasn’t there before, or does it simply replace something human with something digital and call that an improvement?
Does it adapt: does it respond to who you actually are, what you actually need, in the moment you actually need it?
This system fails all three.
It does not assist. It places more demands on Alex than the phone call it replaced. It does not augment their care. It has removed the human relationship that was the most important part of that care. And it does not adapt. It treats Alex, a person with a clinically diagnosed mental health condition, in exactly the same way it treats everyone else.
Treating everyone the same is not equality. Sometimes it is the opposite.
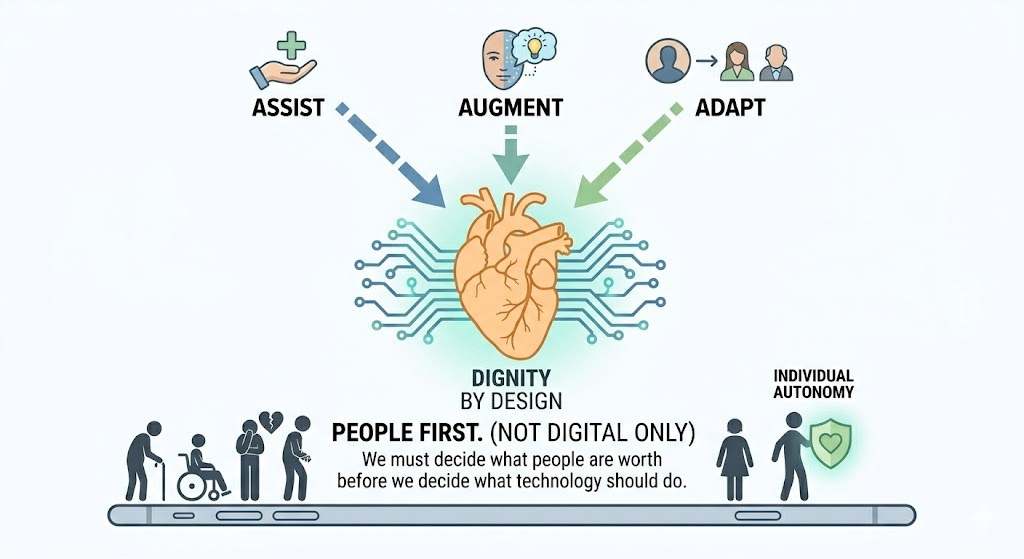
People First
There is a broader point here that the technology industry is not yet comfortable making.
The move to digital-first services in healthcare, in banking, in government, in almost every area of public life, is happening faster than our understanding of who gets left behind. We talk about the digital divide as though it is simply a question of access. Who has a smartphone. Who has broadband. Who can afford a data plan.
But there is another divide, quieter and harder to measure. It is the gap between people for whom digital systems work as intended, and people for whom those same systems are a source of genuine harm. People with cognitive conditions. People with anxiety. People who are older, or less confident, or simply having a bad day in a way the system cannot see and was never built to accommodate.
We are moving to digital only. And we are doing it before we have answered the most important question.
Digital for whom?
Trust lost is hard to regain.
Alex still gets the medication. Most of the time. But something has changed that a prescription cannot fix.
Trust in the surgery is gone. The relationship built over years with a doctor now sits behind ten screens and a system that does not know Alex’s name in any meaningful sense. The feeling, in their own words, is of being a case number.
The technology did not intend this. But it caused it. And intention, in the end, is no comfort to the person on the wrong side of the screen.
We have a choice about how we build these systems. We can continue to build for the average and accept that the people who fall outside that average will simply have to manage. Or we can decide that technology which does not adapt to the individual is un-finished technology. It is a draft. And we owe it to people like Alex to keep working on it until it actually fits the human being in front of it.
That is not a technical problem. It is a decision about what we think people are worth.
Whilst the name Alex is fictitious, their story is not - it is 100% real and is not unique. Versions of it are playing out every day, in surgeries, job centres, banks, and council offices across the country. The details change. The experience doesn’t.
So I’d like to leave you with four questions. Not rhetorical ones, genuine ones, worth sitting with.
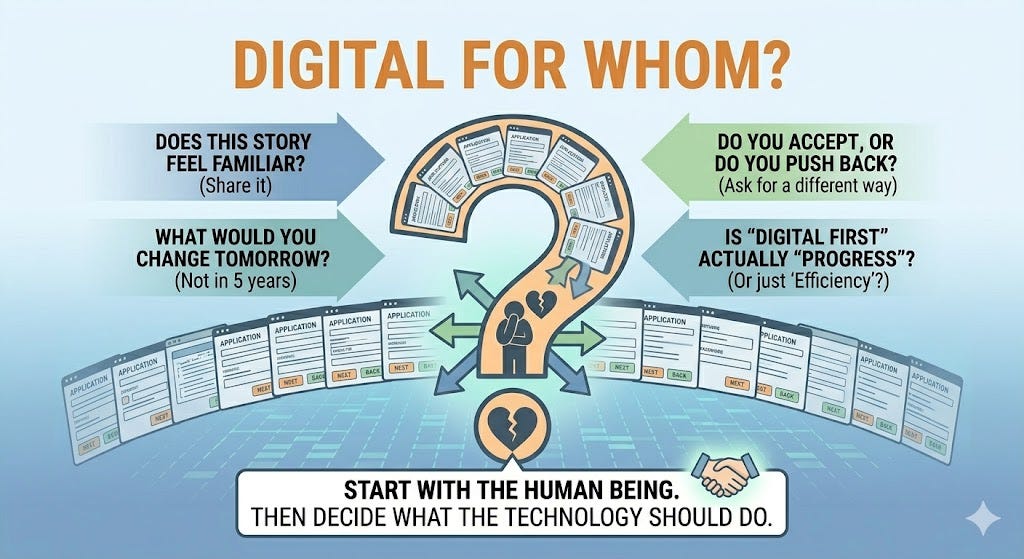
Does this story feel familiar? Perhaps it happened to you, or to someone you know. If it does, that matters. These experiences rarely make the headlines but they shape people’s lives in ways that statistics never capture. If you have a story, share it. The more visible these experiences become, the harder they are to ignore.
If you work with technology - designing it, commissioning it, deploying it - what would you change tomorrow if you could? Not in five years, not after the next funding round. Tomorrow. The answer to that question is usually simpler than we pretend, and the fact that it hasn’t been done yet is itself worth examining.
If you use these systems - as a patient, a customer, a citizen - do you accept what you’re given, or do you push back? Asking for a different way is not unreasonable. It is, in fact, exactly the kind of pressure that eventually changes things.
And finally, the bigger question underneath all of it. Is digital first actually the right approach or have we confused efficiency with progress? Perhaps the answer isn’t digital first, or analogue first, but something more honest: people first. Start with the human being. Then decide what the technology should do.
That shift in thinking costs nothing. What comes after it might change everything.
If this piece resonated with you, I’d welcome your thoughts in the comments.
I am a technology strategist and author focused on the intersection of technology, ethics, and human purpose. My books include The Next Evolution, The Cognitive Crucible, and The Shadow System.