
The Instruction In The Injection
mRNA can teach the immune system to hunt cancer. The harder question is who gets access.

In the spring of 2023, a patient at Memorial Sloan Kettering Cancer Center in New York received an injection that had been made specifically for them. The sequence of molecules inside it had been designed using a biopsy of their own tumour. No one else in the world would receive exactly this treatment. The vaccine’s job was not to prevent a disease — it was to teach the immune system to recognise and destroy cancer cells that were already there.
The patient had pancreatic cancer. Pancreatic cancer kills around 87% of the people diagnosed with it within five years. It is resistant to most forms of treatment. The immune system usually does not recognise it as a threat. The mRNA vaccine was attempting to change that.
Three years later, the patient had not relapsed. In the trial they had been part of, vaccine-induced immune responses were still detectable in the blood — a signal that the immune system was still, years on, watching for the cancer to return. This is not a cure. It is not even yet a proven treatment outside of trials. But it is the kind of result that changes what researchers believe is possible.
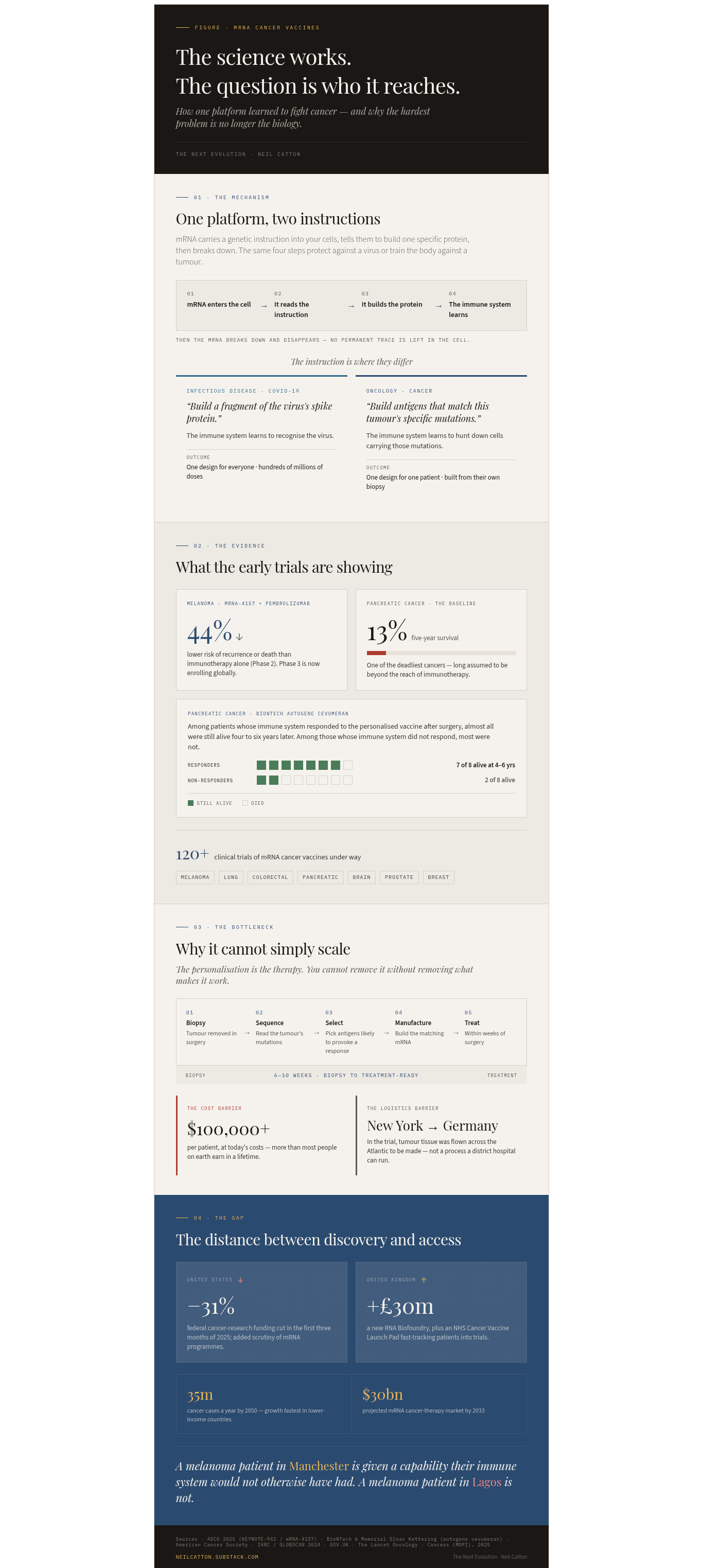
The technology making it possible is the same one that protected hundreds of millions of people against COVID-19. mRNA — messenger ribonucleic acid — carries genetic instructions into cells, tells them to produce a specific protein, and then disappears. For infectious disease, the instruction was: produce a fragment of the virus’s spike protein, and let the immune system learn to recognise it. For cancer, the instruction is more personal: produce antigens that match the specific mutations in this patient’s tumour, so the immune system learns to hunt down cells carrying those mutations. The concept is the same.
Beyond COVID: what mRNA can and cannot do
The COVID vaccines demonstrated something that decades of laboratory research had suggested but never proved at scale: mRNA can be manufactured rapidly, delivered safely into human cells, and used to produce a protein the body has never encountered before. Before 2020, no mRNA medicine had ever been approved for human use. By the end of 2021, hundreds of millions of doses had been administered. The speed was the point — mRNA therapies can be designed in days once the target sequence is known, compared with the months or years required to develop traditional protein-based vaccines.
The platform is now being turned on cancer, autoimmune diseases, and genetic conditions where the body produces too little or too much of a particular protein. The logic is the same in each case: if you can specify the instruction, you can produce the protein.
Cancer is the most advanced frontier. There are now more than 120 clinical trials of mRNA cancer vaccines currently under way, targeting melanoma, lung, colorectal, pancreatic, brain, prostate and breast cancers, among others. The most significant results to date come from melanoma. A personalised mRNA vaccine called mRNA-4157, developed by Moderna in collaboration with the immunotherapy drug pembrolizumab, reduced the risk of recurrence or death by 44% compared to pembrolizumab alone in a Phase 2 trial. Patients given the combination were less likely to see their cancer return at five years than those who received the immunotherapy drug on its own. Phase 3 trials are now enrolling globally.
mRNA carries instructions into cells. For COVID, the instruction was: learn to recognise a virus. For cancer, the instruction is: learn to hunt down cells carrying these specific mutations.
The pancreatic cancer results are more tentative but potentially more significant, given how few treatment options exist. BioNTech’s personalised vaccine, autogene cevumeran, in combination with chemotherapy and immunotherapy, produced durable immune responses in pancreatic cancer patients — and in follow-up data published in 2025 and 2026, seven of the eight patients whose immune systems responded to the vaccine were still alive four to six years after surgery. Of the eight who did not respond, only two were. Pancreatic cancer’s resistance to immunotherapy had long been assumed to be near-absolute. These results suggest it may be conditional.
Beyond cancer, mRNA is in clinical trials for influenza, HIV, tuberculosis, and a range of rare genetic conditions where specific proteins are absent or dysfunctional. The questions are about speed, cost, and who gets access.
The personalisation problem
The most powerful version of mRNA cancer therapy is also its most limiting feature. A personalised vaccine — one designed around the specific mutations in a single patient’s tumour — is, by definition, a product that cannot be manufactured at scale. It requires a biopsy, genomic sequencing to identify which mutations are present and likely to trigger an immune response, computational modelling to select the right antigens, and then manufacture of the mRNA sequence that encodes them. This has to happen quickly enough to be clinically relevant, which in practice means within weeks of surgery.
The current manufacturing timeline for a personalised mRNA vaccine runs between six and ten weeks from biopsy to treatment-ready product, depending on the programme, and researchers are working to compress it further. The logistics are not incidental to the clinical result. In the BioNTech pancreatic trial, tumour tissue removed in New York was shipped to manufacturing facilities in Germany. The time between tissue leaving the body and the vaccine being ready had to be minimised. This is not a process that transfers easily to a district general hospital in the English Midlands, or a regional cancer centre in West Africa.
Cost is the other constraint. Manufacturing a personalised mRNA cancer vaccine currently costs upwards of $100,000 per patient. That figure reflects the early-stage nature of the technology — the expectation is that automation and manufacturing improvements will bring it down — but it is the figure that exists today, not the figure that might exist in 2035. For a health system trying to decide where to invest limited resources, a treatment that costs more than most people in the world earn in a lifetime, and that has not yet completed Phase 3 trials, is not an immediate commissioning priority.
A personalised cancer vaccine is designed around a single patient’s tumour mutations. That is its power. It is also why manufacturing it at scale, at a cost that health systems can absorb, is the defining challenge.
There is a further complication that does not feature in most of the coverage of mRNA therapeutics, but is directly relevant to where the technology goes next. In the United States, federal investment in mRNA vaccine research — which underpins much of the academic pipeline — was significantly cut in 2025. The National Cancer Institute saw funding reductions of around 31% in the first three months of that year. Research programmes specifically developing mRNA cancer vaccines faced additional scrutiny from the Department of Health and Human Services. The political pressure on mRNA technology in the US, driven by anti-vaccine sentiment that predated and outlasted COVID, is a genuine threat to the public research infrastructure on which the field depends.
The UK has moved in the opposite direction. In August 2025, the government announced £30 million for a UK RNA Biofoundry specifically to accelerate RNA therapy development. The Cancer Vaccine Launch Pad, a collaboration between the NHS and BioNTech, is fast-tracking thousands of patients into mRNA cancer vaccine trials targeting lung, breast, head and neck, and other cancers. The global market for mRNA cancer therapies is projected to reach $30 billion by 2033. The investment is arriving. Whether it arrives equitably — or concentrates in the health systems that can most readily afford it — is the question that will define the technology’s impact.
The distance between discovery and access
The patient at Memorial Sloan Kettering who received the pancreatic cancer vaccine in 2023 lived close to one of the world’s best-funded cancer research institutions, in a country with a health insurance system that covers experimental treatments for some patients in some circumstances, and was enrolled in a clinical trial with costs covered by the research programme. These were not incidental conditions. They were why that patient was treated and not someone else.
Pancreatic cancer does not concentrate in wealthy neighbourhoods. Neither does melanoma, lung cancer, glioblastoma, or any of the other cancers now being targeted by mRNA trials. But the trials are running almost exclusively in high-income countries, at major academic medical centres, with manufacturing infrastructure that does not exist in the places where cancer burden is rising fastest. By 2050, global cancer incidence is projected to reach 35 million cases per year — a significant portion of that growth driven by population ageing in low and middle-income countries. The treatments being developed now may arrive in those countries decades after they become available in New York or London, if they arrive at all.
This is not unique to mRNA. It is the pattern of almost every major therapeutic innovation. But mRNA was supposed to be different — its manufacturing speed and relative simplicity were explicitly cited, during the pandemic, as reasons to believe it could close the gap between rich and poor countries in access to medicines. That aspiration now needs to be tested against the reality of personalised cancer treatment, where the manufacturing process is the opposite of simple, the cost per patient is the opposite of affordable, and the regulatory frameworks governing it are only beginning to be developed.
My Opinion
The field’s working assumption is that personalised mRNA vaccines will become affordable as manufacturing scales. I think that is optimistic in a way that lets the field avoid a harder question.
A vaccine designed around one patient’s specific tumour mutations is not a product that scales the way a platform does. The personalisation is the therapy. You cannot remove it without removing what makes it work.
If the goal is equitable treatment, the investment needs to run in two directions simultaneously: into making personalised approaches cheaper and faster for the patients who can access specialist centres, and into shared-antigen mRNA approaches that target common mutations across large patient populations. The second track is less scientifically compelling. It is more likely to reach the person in Lagos.
The field rarely discusses this openly. The personalised vaccine is the story. Population-level mRNA is not. That asymmetry in attention is worth examining.
What the technology can and cannot yet do
mRNA cancer therapy helps the body do something it already knows how to do — mount an immune response — but has failed to do against a tumour that has learned to hide. The technology does not replace the immune system. It gives it better information. That is precisely the kind of assistance that medicine has sought for decades in treating cancers that resist other approaches. The question is not whether it works in the biology. The question is whether it works for the people who need it.
A melanoma patient in Manchester enrolled in a Cancer Vaccine Launch Pad trial is being given a capability their immune system would not otherwise have had. A melanoma patient in Lagos is not. The science adds something genuinely new. The system around it does not yet extend that addition to the people most likely to be without other options.
Personalised mRNA vaccines are, in the narrow technical sense, the most individual cancer treatment ever designed — each one built for one person, from that person’s own tumour biology. The treatment is exquisitely adapted to the biology. It is not yet adapted to the world.
The questions the science leaves open
The biology is not the hardest part. These are not questions about whether the technology works — the early evidence says it does. They are questions about investment, access, geography, and design: about who makes the decisions that will determine whether the science reaches everyone it could reach, or only the people who were already closest to it.
The UK Cancer Vaccine Launch Pad is enrolling NHS patients in mRNA cancer trials right now. If you or someone you know has been affected by one of the cancers being targeted — melanoma, lung, breast, head and neck — do you know how to find out whether a trial is relevant?
The manufacturing cost of a personalised mRNA vaccine is currently around $100,000 per patient. What would it take — in automation, in manufacturing scale, in public investment — to bring that number to one that health systems in lower-income countries could absorb?
The US has cut federal investment in mRNA research. The UK has increased it. What does it say about the future geography of cancer treatment that the direction of public investment in the science varies so sharply between countries?
The patient in New York survived because they were in the right place, enrolled in the right trial, at the right time. What would it take to design a version of this technology — and the healthcare system around it — where that sentence did not define who gets treated?
The mRNA platform can encode almost any protein the body can produce. The immune system can, it turns out, be taught to recognise almost any mutation cancer can generate. These two facts together are the reason that researchers who have spent their careers treating pancreatic cancer — a disease long described as an almost certain death sentence — are now using words like ‘paradigm shift’.
The science is moving faster than most of the systems around it. The history of medical innovation suggests the systems do not catch up on their own.
Sources and references
Pancreatic cancer survival rate: Pancreatic Cancer Action Network press release, 2025: five-year relative survival rate stalls at 13%. American Cancer Society, Survival Rates for Pancreatic Cancer, 2025. cancer.org
mRNA-4157 melanoma trial (KEYNOTE-942): Individualised neoantigen therapy mRNA-4157 (V940) plus pembrolizumab versus pembrolizumab monotherapy in resected melanoma: a randomised, phase 2b study. The Lancet, 2023. Updated three-year results presented at ASCO, 2025. Five-year recurrence-free survival data: CancerNetwork, 2025.
BioNTech autogene cevumeran — pancreatic cancer: Three-Year Phase 1 Follow-Up Data, BioNTech press release, 2025. Updated follow-up (4–6 years): Memorial Sloan Kettering Cancer Center news release; reported in CNN Health, April 2026. AACR Annual Meeting 2025: immune response correlates with clinical benefit in pancreatic cancer patients.
US federal cancer research funding cuts: US Senate Minority Staff report, May 2025: federal cancer research funding reduced by approximately 31% in the first three months of 2025. Reported in Axios, PBS NewsHour, OncLive (May 2025).
UK RNA Biofoundry: GOV.UK press release, 28 August 2025: £29.6 million investment in UK RNA Biofoundry at CPI’s RNA Centre of Excellence, Darlington. gov.uk
Global cancer incidence projections to 2050: IARC / GLOBOCAN 2024 projections: global cancer incidence projected to reach 35 million cases annually by 2050, a 77% increase from 2022. Reported by UN News, February 2024. (Note: the Global Burden of Disease Study 2023 uses a lower estimate of 30.5 million; the IARC figure is the more widely cited projection.)
mRNA cancer vaccine market projection ($30 billion by 2033): Noted in commentary published in The Lancet Oncology, 2025, drawing on market research projections. The underlying figure originates from commercial market research.
Manufacturing cost and timeline: Manufacturing costs upwards of $100,000 per patient: reported across multiple clinical development sources including Scientific American (2025) and RNA cancer vaccine pipeline reviews (PMC, 2025). Timeline of 6–10 weeks from biopsy to treatment-ready product: Moderna manufacturing data; autogene cevumeran trial documentation showing approximately 9-week average for the BioNTech pancreatic cancer programme.
120+ clinical trials: Current Progress and Future Perspectives of RNA-Based Cancer Vaccines: A 2025 Update. Cancers (MDPI), May 2025. PMC12153701
Cancer Vaccine Launch Pad: NHS England / BioNTech Cancer Vaccine Launch Pad: fast-tracking patients into mRNA cancer vaccine trials targeting melanoma, lung, breast, head and neck, and other cancers. nhs.uk
You’re reading The Next Evolution by Neil Catton, articles that explore the human world and the intersection of technology, they try and ask difficult questions - not to scare - but to inform. If someone forwarded this to you, you can subscribe free at neilcatton.substack.com.
Neil Catton is the author of The Next Evolution, The Cognitive Crucible and The Shadow System - available on Amazon, and writes at the intersection of technology, ethics, and human purpose.